Working Diagnosis:
The working diagnosis for this athlete was persistent atrial fibrillation with severe sporadic aortic root dilation.
Treatment:
He was started on anticoagulation with apixaban. 3 weeks later, he underwent a successful transesophageal echocardiogram with direct current cardioversion and was discharged in normal sinus rhythm with no recurrence of palpitations. He continued on anticoagulation for 4 weeks after cardioversion and remained in sinus rhythm on subsequent electrocardiograms. He was not started on long-term anticoagulation due to having a CHADS2VASC score of zero. Two months later, he underwent a successful sternotomy with valve-sparing aortic root replacement with coronary ostial reimplantation, ascending aorta replacement, left atrial appendage amputation, and pulmonary vein ablation. He was started on 81 milligrams of aspirin daily indefinitely, metoprolol tartrate 12.5 milligrams twice daily for atrial fibrillation prevention for 3 months post-op, and was given furosemide 20 milligrams to be used once daily as needed for weight gain of 3 pounds in one day or 5 pounds in one week. He was also started on amiodarone, but this was discontinued due to a prolonged post-operative QTc of greater than 500. His post-operative course was complicated by pericarditis, which resolved with 30 days of colchicine 0.6 milligrams daily. His pre-operative and post-operative course was also complicated by adjustment disorder, which was well controlled with escitalopram 5 milligrams daily.
Outcome:
This athlete was restricted from all basketball-related activity indefinitely. He started a formal cardiac rehabilitation program and was permitted to perform moderate aerobic exercise as tolerated. At follow-up cardiology appointments, he remained asymptomatic post-operatively, completed metoprolol tartrate, and was tolerating low-dose aspirin without side effects. He had not needed any doses of furosemide. He had not experienced a recurrence of atrial fibrillation. He will have regular follow-up with cardiology for long-term imaging surveillance 6-12 months post-operatively and every 5 years after that. He had no plans to return to playing basketball in the future.
Author's Comments:
Athletes have a higher risk of developing atrial fibrillation than non-athletes, particularly those under age 40 who participate in mixed-type sports like basketball, football, or soccer (3). While the exact mechanisms remain unclear, atrial fibrillation in athletes is thought to result from the interaction of three main components:(1) a trigger--such as stimulant use, atrial ectopy, or supplement use; (2) a substrate--such as genetic predisposition, inflammation, fibrosis, or structural remodeling; and (3) a modulator--such as autonomic nervous system activation or electrolyte disturbances (4). In our athlete's case, we hypothesize that his aortic root dilation may have contributed to atrial fibrillation by promoting atrial remodeling or exerting mechanical pressure on the pulmonary veins, altering electrical conduction.
Considering this athlete's competitive level and the goal to preserve athletic performance, rhythm control was achieved with cardioversion rather than antiarrhythmic medication or rate control. The 2023 American Heart Association/American College of Cardiology guidelines support catheter ablation as a preferred option in athletes with atrial fibrillation, given its high success rate and minimal impact on exercise capacity (5). In contrast, medications like beta blockers can impair performance and may require a therapeutic use exemption depending on the athlete's level of competition. Given the concurrent need for surgical intervention for aortic root dilation in this athlete, cardioversion was chosen over ablation as the initial approach to minimize procedural burden and optimize surgical outcomes by restoring sinus rhythm prior to thoracotomy.
Thoracic aortic root dilation is a rare but potentially fatal cardiovascular condition in young athletes. It tends to present earlier than other aortopathies, such as abdominal aortic aneurysms, and is more commonly associated with heritable disorders like Marfan syndrome, Loeys-Dietz syndrome, vascular Ehlers-Danlos syndrome, or congenital anomalies such as bicuspid aortic valve. Traditional cardiovascular risk factors, smoking, hypertension, diabetes, are less commonly implicated in this population(6). Aortic root diameter varies with age, sex, height, and weight; males and taller individuals tend to have larger diameters, and the aortic root typically enlarges about 1 mm per decade(1).
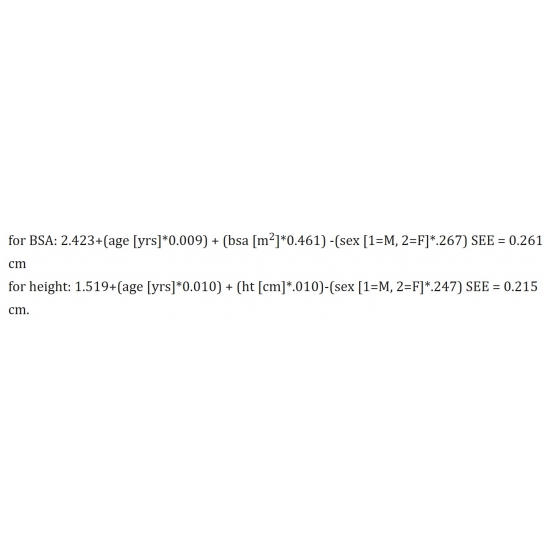
Although intense athletic training can mildly increase aortic root size, by an estimated 3.2 mm, this level of dilation is not considered pathological(7). Our athlete's aortic root dilation exceeded what would be expected from physiologic remodeling alone. His aortic root z-score, calculated at the sinus of Valsalva, was significantly elevated at +7.90 (normal -2 to +2). While z-scores have traditionally been used in pediatric populations, newer studies incorporating age into adult z-score equations have improved their utility Case Photo #6 (1). Given the athlete's age (22), his z-score is unlikely to reflect age-related changes and instead indicates pathologic enlargement.
In 2022, the American Heart Association/American College of Cardiology updated guidelines for the management of aortopathies. For sporadic (non-genetic) aortic root dilation, they recommended medication management including blood pressure control with a beta blocker or angiotensin converting enzyme inhibitor (target less than 130/80 mmHg), considering statin therapy even in the absence of atherosclerosis, low-dose aspirin (particularly if atherosclerosis is present), and smoking cessation (6,7,8). This athlete was started on a beta blocker post-ablation for atrial fibrillation prevention and was able to discontinue it after three months due to well-controlled blood pressure and no recurrence of arrhythmia. He remained on low-dose aspirin but had not started a statin given his age.
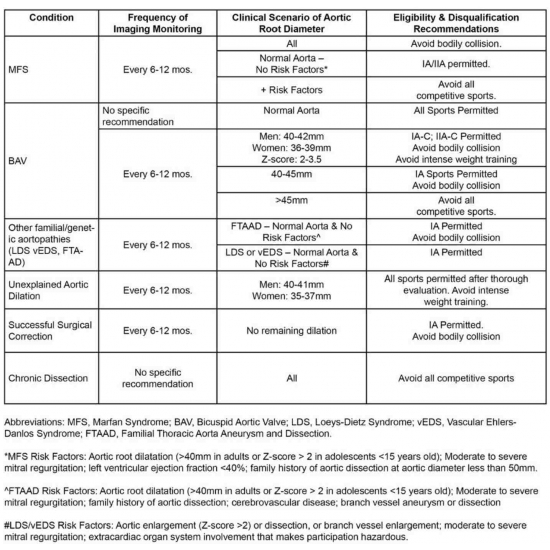
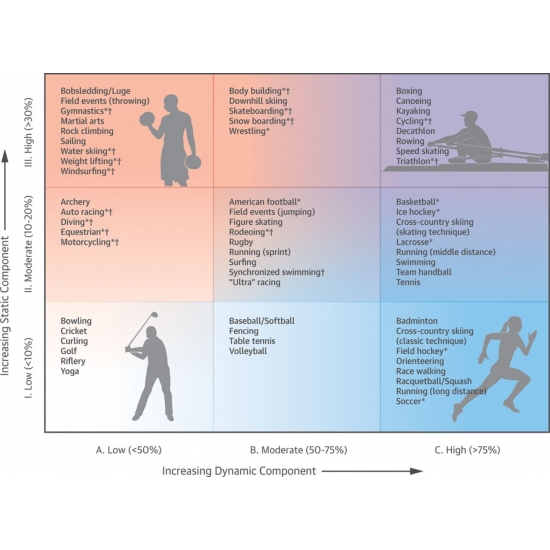
This athlete met multiple American Heart Association/American College of Cardiology guidelines for surgical intervention including: (1) symptoms attributable aortic dilation (palpitations, atrial fibrillation), (2) aortic diameter at least 5.5 centimeters, and (3) documented growth of at least 0.5 centimeters in a single year or 0.3 centimeters in two consecutive years.6,8,9 Following surgical repair, he began a formal cardiac rehabilitation program and performed moderate-intensity aerobic exercise as tolerated in accordance with their recommendations. They also recommend avoidance of isometric exercise and bodily collision(10). Athletes with unexplained aortic root dilation not meeting surgical criteria may still participate in all sports with regular imaging surveillance. Following surgical repair, participation is restricted to low-static, low-dynamic (Type IA) sports Case Photo #7 , which impose minimal cardiovascular stress, examples include golf and bowling Case Photo #8 (11-12).
Though these restrictions remain the standard, emerging data suggest endurance exercise (marathons or triathlons) may carry low risk after thoracic aortic repair (13). Anecdotally, three NBA players, Chris Wilcox, Ronny Turiaf, and Jeff Green, returned to high-level competition after undergoing the same surgery, following careful monitoring and individualized risk-benefit discussions. Remarkably, all three shared the court during a 2013 game post-repair (14-16).
At present, our athlete was progressing through cardiac rehabilitation with no recurrence of symptoms. He will undergo imaging surveillance at one year post-repair and every five years thereafter. He remained asymptomatic and had no immediate plans to return to competitive basketball, though shared decision-making will guide future activity.
Editor's Comments:
This case highlights the importance of the preparticipation exam prior to sports participation even if previously evaluated at other institutions. It discusses the evaluation and treatment of atrial fibrillation and aortopathies in athletes. Athletes carry a higher risk of developing atrial fibrillation than their non athletic peers which is usually a result from triggers such as stimulant or supplement use, a substrate such as genetic predisposition, fibrosis or structural remodeling or a modulator such as autonomic nervous system activation or electrolyte issues. Ablation is the preferred treatment in athletes due to the high success rate and limited impact on exercise capacity. Thoracic aortic root dilation is a rare but potentially fatal aortopathy that may be associated with congenital heritable disorders. Nonsurgical treatment for aortic root dilation includes blood pressure control with a beta blocker or angiotensin converting enzyme inhibitor, statin therapy, low-dose aspirin, and smoking cessation and allows for participation in all sports with regular imaging surveillance. Surgically treated aortopathies are only allowed to participate in low static and low dynamic sports such as golf and bowling.
References:
1.Devereux RB;de Simone G;Arnett DK;Best LG;Boerwinkle E;Howard BV;Kitzman D;Lee ET;Mosley TH;Weder A;Roman MJ; "Normal Limits in Relation to Age, Body Size and Gender of Two-Dimensional Echocardiographic Aortic Root Dimensions in Persons ≥15 Years of Age." The American Journal of Cardiology, U.S. National Library of Medicine, July 2012, pubmed.ncbi.nlm.nih.gov/22770936/.
2."Z-Score for Adults." Marfan Foundation, 16 Nov. 2021, marfan.org/dx/z-score-adults/.
3.Newman W, Parry-Williams G, Wiles J, et al. Risk of atrial fibrillation in athletes: a systematic review and meta-analysis. British Journal of Sports Medicine 2021;55:1233-1238.
4.Turagam MK, Flaker GC, Velagapudi P, Vadali S, Alpert MA. Atrial Fibrillation In Athletes: Pathophysiology, Clinical Presentation, Evaluation and Management. J Atr Fibrillation. 2015 Dec 31;8(4):1309. doi: 10.4022/jafib.1309. PMID: 27957228; PMCID: PMC5135187.
5.Joglar JA, Chung MK, Armbruster AL, Benjamin EJ, Chyou JY, Cronin EM, Deswal A, Eckhardt LL, Goldberger ZD, Gopinathannair R, Gorenek B, Hess PL, Hlatky M, Hogan G, Ibeh C, Indik JH, Kido K, Kusumoto F, Link MS, Linta KT, Marcus GM, McCarthy PM, Patel N, Patton KK, Perez MV, Piccini JP, Russo AM, Sanders P, Streur MM, Thomas KL, Times S, Tisdale JE, Valente AM, Van Wagoner DR; Peer Review Committee Members. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024 Jan 2;149(1):e1-e156. doi: 10.1161/CIR.0000000000001193. Epub 2023 Nov 30. Erratum in: Circulation. 2024 Jan 2;149(1):e167. doi: 10.1161/CIR.0000000000001207. Erratum in: Circulation. 2024 Feb 27;149(9):e936. doi: 10.1161/CIR.0000000000001218. Erratum in: Circulation. 2024 Jun 11;149(24):e1413. doi: 10.1161/CIR.0000000000001263. PMID: 38033089; PMCID: PMC11095842.
6."2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines." American College of Cardiology, Dec. 2022, www.jacc.org/doi/abs/10.1016/j.jacc.2022.08.004.
7.Meagher, Sean P, and Alan C Braverman. "CV Sports Chat: Dilated Aortas in Athletes." American College of Cardiology, 9 Sept. 2024, www.acc.org/latest-in-cardiology/articles/2024/09/09/10/21/cv-sports-chat-dilated-aortas-in-athletes.
8."2022 ACC/AHA Aortic Disease Guideline Key Perspectives: Part 1 of 2." American College of Cardiology, 2 Nov. 2022, www.acc.org/Latest-in-Cardiology/ten-points-to-remember/2022/11/01/12/17/2022-guideline-on-aortic-disease-1-gl-ad.
9."2022 ACC/AHA Aortic Disease Guideline Key Perspectives: Part 2 of 2." American College of Cardiology, 2 Nov. 2022, www.acc.org/Latest-in-Cardiology/ten-points-to-remember/2022/11/01/12/21/2022-guideline-on-aortic-disease-2-gl-ad.
10.Braverman AC, Harris KM, Kovacs RJ, Maron BJ; American Heart Association Electrocardiography and Arrhythmias Committee of Council on Clinical Cardiology, Council on Cardiovascular Disease in Young, Council on Cardiovascular and Stroke Nursing, Council on Functional Genomics and Translational Biology, and American College of Cardiology. Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 7: Aortic Diseases, Including Marfan Syndrome: A Scientific Statement From the American Heart Association and American College of Cardiology. Circulation. 2015 Dec 1;132(22):e303-9. doi: 10.1161/CIR.0000000000000243. Epub 2015 Nov 2. PMID: 26621648.
11.Hsu, Jeffrey J, and Dermott J Phelan. "Exercise in Aortopathy: How Should We Counsel Our Patients?" American College of Cardiology, 7 Aug. 2020, www.acc.org/latest-in-cardiology/articles/2020/08/07/08/07/exercise-in-aortopathy.
12.Levine BD, Baggish AL, Kovacs RJ, Link MS, Maron MS, Mitchell JH; American Heart Association Electrocardiography and Arrhythmias Committee of Council on Clinical Cardiology, Council on Cardiovascular Disease in Young, Council on Cardiovascular and Stroke Nursing, Council on Functional Genomics and Translational Biology, and American College of Cardiology. Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 1: Classification of Sports: Dynamic, Static, and Impact: A Scientific Statement From the American Heart Association and American College of Cardiology. Circulation. 2015 Dec 1;132(22):e262-6. doi: 10.1161/CIR.0000000000000237. Epub 2015 Nov 2. PMID: 26621643.
13."Endurance Exercise Following Ascending Thoracic Aortic Aneurysm Resection in Bicuspid Aortic Valve Aortopathy | Congenital Defects | Jama Cardiology | Jama Network." American College of Cardiology, Mar. 2022, jamanetwork.com/journals/jamacardiology/fullarticle/2793311.
14."Ronny Turiaf's Heart Surgery Replaces Aortic Root, Preserves Valve." Heart Valve Surgery, Sept. 2020, www.heart-valve-surgery.com/ronny-turiaf-aorta-valve.php.
15.Maine, D'Arcy. "Jeff Green's Road to the Finals Couldn't Have Been Easy -- Trust Me, I Know." ESPN, ESPN Internet Ventures, 31 May 2018, www.espn.com/nba/story/_/id/23658177.
16."Three of Hearts: Turiaf, Green, Wilcox Share Survival Story." NBC Sports Boston, NBC Sports Boston, 4 Feb. 2013, www.nbcsportsboston.com/nba/boston-celtics/three-of-hearts-turiaf-green-wilcox-share-survival-story/316926/.
Return To The Case Studies List.




























{kind=link}
{kind=link}
{kind=link}