Working Diagnosis:
Recalcitrant lateral epicondyle tendinopathy
Treatment:
He received ultrasound-guided percutaneous needle fenestration of the calcifications and tear, platelet-rich plasma injection, and a specific post-PRP rehabilitation protocol that included eccentric exercises.
PROCEDURE
After explaining the risks and benefits of the procedure and answering all questions, consent was obtained. The patient was prepared for a venipuncture of one of the veins in the antecubital fossa of the left arm, and approximately 20 ml of whole blood were drawn into a syringe containing 2 ml of anticoagulant citrate dextrose solution, formula A (ACD-A). This blood was processed personally by the attending physician at the clinic using a SmartPReP APC system processing machine following the SmartPReP Office Protocol. Approximately 4 ml of platelet-rich plasma concentrate were collected. No activators were used.
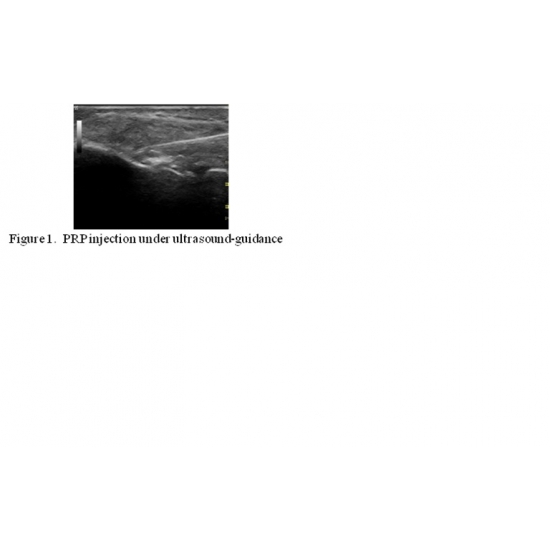
The patient was positioned on the examination table and the right lateral elbow was cleaned in a sterile manner. Under ultrasound guidance, 1ml of 2% lidocaine was injected into the surrounding soft tissue for local anesthesia. Then, under ultrasound guidance, the calcific changes at the attachment of the common extensor tendon into the lateral epicondyle were fenestrated with the needle multiple times. The tear was then fenestrated too. Finally, the PRP concentrate was infused both at the site of the calcifications as well as at the site of the partial midsubstance tear. Case Photo #1 . The entire platelet-rich plasma concentrate was visualized in the ultrasound screen going into the correct tissue spaces. The procedure took 45 minutes to complete, including the processing and collection of the PRP.
Post-procedure instructions were given to the patient, including a specific rehabilitation protocol. [Table 1]. He was advised to avoid non-steroidal anti-inflammatory medications, including selective Cox-2 inhibitors. For post-operative pain or discomfort, an ice pack topically and acetaminophen were recommended. The patient completed the rehabilitation protocol accordingly without any complications or setbacks.
Outcome:
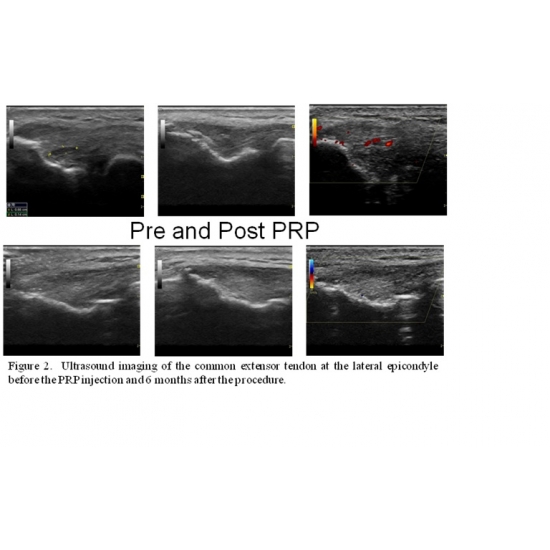
Three months after the procedure, the patient reported more than 75% improvement in his symptoms. At six months, he reported more than 95% improvement. A follow-up ultrasound evaluation showed complete resolution of the partial tendon tear, no calcifications at the enthesis of the tendon, and no intra-tendinous vascularization. Case Photo #2 At a follow-up visit, he stated "I have achieved a near complete elimination of pain, with only minimal soreness at times after playing tennis or strenuous activity for more than an hour. I feel like my elbow has the resiliency now to recover quickly from any discomfort or minor flare up of pain."� At 12 months after the procedure, he indicated that he was back to playing tennis twice a week and was able to do several activities completely pain-free. He stated âI wish someone would have talked to me about PRP a year ago after I had failed the first steroid injection and physical therapy."�
Author's Comments:
Tendon injuries are estimated to comprise between 30% to 50% of all sports-related injuries.[1] Tendinopathy of the extensor muscles inserting in the lateral elbow is commonly seen in patients who perform strong gripping or repetitive wrist flexion and extension movements.[2] Lateral epicondylitis is the most commonly diagnosed condition of the elbow, affecting approximately 1% to 3% of the population, and occurs in mostly middle-aged patients.[3,4] The tissue healing of these injuries may become impaired with time by the development of tissue fibrosis.[5] In addition, collagen degeneration, neovascularization, intra-tendinous calcifications, and thickening of the tendon may delay the maturation of a healing tendon.[6,7]
Patients with chronic tendon injuries usually try various therapeutic options, including non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroid injections, nitric oxide patches, immobilization, cryotherapy, heat, massage, phonophoresis, stretching, strengthening, electric-stimulation, dry needling, acupuncture, rest, and eccentric exercises. Despite these efforts, some patients continue reporting significant pain that impairs them from performing functional activities at their full potential. One of the most frequently used treatments for the pain associated with tendinopathies is anti-inflammatory drugs such as NSAIDs including selective cyclooxygenase-2 (COX-2) inhibitors and corticosteroid injections. However, these treatment options have recently been questioned. A study on the effect of ibuprofen on rat Achilles tendon cells showed increased activity of collagen-degrading enzymes, suggesting a detrimental effect of ibuprofen over the mechanism for tendon healing.[8] In vitro and in vivo experiments showed that NS-398, a specific COX-2 inhibitor, inhibited the proliferation and maturation of differentiated myogenic precursor cells, suggesting a detrimental effect on skeletal muscle healing.[9]
Studies on corticosteroid injections for lateral epicondylitis show positive short-term results, but frequent relapses and no significant difference to placebo or physiotherapy at 1 year.[10,11] In addition, corticosteroid injections have resulted in tendon rupture in several cases of Achilles tendinopathy.[12] Some studies suggest that non-pharmacologic options such as eccentric exercises are more effective than anti-inflammatory drugs for chronic tendinopathies.[13,14] They recommend eccentric exercises as one of the most promising treatments for tendinopathies.
Platelet-rich plasma (PRP) injection has been introduced as a safe alternative for treating chronic tendinopathies and carries minimal risk. Its use for musculoskeletal injuries has increased recently, given its safety and availability for outpatient preparation and delivery.[15] PRP is considered an ideal autologous blood product that promotes the body's own natural healing.[16] This concentrate has been used for over 25 years in the clinical setting of oral and maxillofacial surgery, otorhinolaryngology, plastic surgery, and general surgery, with multiple case-series reports showing overall improvement in soft tissue healing.[17-19] It has recently become popular in the management of musculoskeletal injuries, based on in-vitro studies reporting an enhancement of the recruitment, proliferation, and differentiation of the cells involved in muscular tissue regeneration.[19,20] Furthermore, case-series reports and small clinical trials have shown successful clinical outcomes in treating different types of musculoskeletal injuries.[19]
PRP is formed by drawing blood from the patient, centrifuging the blood until the red blood cells separate from the platelets and plasma, and then extracting the platelet concentrate from the platelet-rich section of the centrifuged plasma. Platelets are known to carry alpha and dense granules, which contain multiple growth factors and cytokines that promote the wound healing process.[18,21] The five growth factors believed to be the most active during tendon healing are: insulin-like growth factor-I (IGF-I), transforming growth factor beta (TGFbeta), vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and basic fibroblast growth factor (bFGF).[22]
Several of these growth factors have been found to improve muscle regeneration, increase the tensile force in the strained injured muscle, and enhance the tendon healing process.[5,23,24] A study of in vivo use of PRP in human tendon injuries reports that it potentially stimulates cell proliferation, collagen production, and angiogenesis by human tenocytes.[20] Nevertheless, the exact mechanism of action by which PRP initiates the cellular and tissue changes is yet to be fully documented.[21]
Platelet-rich plasma injections are widely accepted by patients since they are produced from the patient's own blood and since the risk of adverse effects other than pain at the injected site are minimal. In a meta-analysis on autologous blood products and PRP injections, no complications were reported in either procedure.[25] In fact, a study on the antibacterial effect of platelet-rich gel in vitro found that the gel inhibited the growth of Staphylococcus aureus and Escherichia coli, making it a reasonable treatment option for infected wounds with delayed healing.[26] This antibacterial property would theoretically reduce the infection rate of the platelet-rich plasma injections. In addition, since PRP is extracted from the patient's own blood, the risk of acquiring a transmitted blood-born infection or suffering an anaphylactic reaction is extremely rare.[16] It also carries a significantly lower cost than surgical management, which is frequently the last resort for chronic tendinopathies. Furthermore, surgical management has not been shown to have promising clinical outcomes due to lack of reliable evidence.[27]
Approximately 87% of the patients with lateral epicondylitis benefit from a combination of physiotherapy and bracing.[28] However, there are a significant number of patients that suffer chronic refractory tendon injuries. A small cohort study on PRP for chronic elbow tendinopathy showed 81% and 93% improvement in pain at 6 months and 2 years, respectively, and recommended considering PRP before referring for surgery.[2] Another study with a larger sample compared PRP (51 patients) to corticosteroid (49 patients) with a one year follow- up and showed a significant difference between PRP and corticosteroid in terms of the visual analog score and Disabilites of Arm, Shoulder, and Hand (DASH) scores. Forty-nine percent of patients in the corticosteroid group versus 73% of the patients in the PRP group had significant improvement in the visual analog scale, and 51% of the patients in the corticosteroid group versus 73% of the patients in the PRP group improved their DASH scores.[16]
Nonetheless, the results were not reproducible in a randomized, double-blind, placebo-controlled trial that compared PRP injection and eccentric exercises versus saline injection and eccentric exercises for Achilles tendinitis. After 24 weeks, both groups showed significant improvement in the VISA-A scale with no statistically significant difference between the two groups.[29] This study looked at cases of acute tendinitis with symptoms for only two months that had not received previous treatment. It is well known that most cases of acute tendinitis will eventually heal. In addition, both the control and the PRP groups performed eccentric exercises, which has been well documented to be beneficial for Achilles tendinitis. Finally, the placebo was actually an active treatment because needling an injured tendon does have a therapeutic effect. PRP is not recommended for acute tendinitis; it is recommended for chronic cases that have failed conservative treatments.
Platelet-rich plasma injections still have a long road ahead before becoming the treatment of choice for chronic tendinopathies. Currently, there is only limited clinical evidence that PRP injections improve function in chronic tendinopathy.[25] This is due to the fact that most of the studies done have been case series reports or case-control studies, frequently with small sample sizes, limiting the generalizability of the findings.[30] Also, the long-term effects of multiple PRP injections have yet to be determined. One meta-analysis explored the relationship between the increased concentration of growth factors in PRP and carcinogenesis. It hypothesized that PRP could not initiate carcinogenesis but could promote it if the PRP is injected near a carcinogenic lesion; the study therefore recommended avoiding PRP on patients with known cancer.[31] An additional question that remains yet to be answered is whether the trauma of the needle entering the tendon multiple times for the delivery of the PRP is actually the main contributor to the healing of the tendon. Various studies on needle fenestration of chronic tendinopathies without corticosteroid injection have reported good to excellent outcomes.[32-34] A study comparing fenestration with and without PRP is warranted.
Despite these limitations, patients with chronic refractory tendinopathies have very few options other than innovative minimally-invasive treatments like PRP. Currently, the best indication for PRP is for chronically painful tendons that have failed to improve despite appropriate conservative treatments. Although the optimal preparation of PRP has not been defined, Mautner et al. suggested that favorable qualities include: higher platelet counts, absence of neutrophils, abundance of lymphocytes, a slightly acidic pH, and ultrasound-guided delivery. The injection should be followed by a specific rehabilitation protocol that includes eccentric exercises to facilitate tendon healing.[35] Certainly, the benefits of PRP seem to outweigh the potential risks. Clinical research with larger sample sizes should take place in order to understand and determine which patient populations would benefit the most from this treatment.
Editor's Comments:
There is emerging evidence for judicious use of platelet-rich-plasma injection in the treatment of tendinopathy.
References:
1. J'rvinen TA, Kannus P, Maffulli N, Khan KM. Achilles tendon disorders: etiology and epidemiology. Foot Ankle Clin. 2005;10(2):255-266.
2. Mishra A, Pavelko T. Treatment of Chronic Elbow Tendinosis with Buffered Platelet Rich Plasma. AM J Sports Med. Nov 2006, 34: 1774-8.
3. Hong QN, Durand MJ, Loisel P. Treatment of lateral epicondylitis: where is the evidence? Joint Bone Spine. 2004;71:369-373
4. Jobe FW, Ciccotti MG. Lateral and medial epicondylitis of the elbow. J Am Acad Orthop Surg. 1994;2:1-8.
5. Kasemkijwattana C, Menetrey J, Bosch P, et al. Use of growth factors to improve muscle healing after strain injury. Clin Orthop Relat Res. 2000;370:272-285.
6. Rees JD, Wilson AM, Wolman RL. Current concepts in the management of tendon disorders. Rheumatology (Oxford). 2006 May;45(5):508-21
7. Maffulli N, Wong J, Almekinders LC. Types and epidemiology of tendinopathy. Clin Sports Med. 2003; 22(4):675-692
8. Tsai WC, Hsu CC, Chang HN, Lin YC, Lin MS, Pang JH. Ibuprofen upregulates expressions of matrix metalloproteinase-1, -8, -9, and -13 without affecting expressions of types I and III collagen in tendon cells. J Orthop Res. 2010 Apr;28(4):487-91.
9. Shen W, Li Y, Tang Y, Cummins J, Huard J. NS-398, a cycloxoygenase-2-specific inhibitor, delays skeletal muscle healing by decreasing regeneration and promoting fibrosis. Am J Pathol. 2005;167(4): 1105-1117.
10. Smidt N, Assendelft WJ, van der Windt DA, Hay EM, Buchbinder R, Bouter LM. Corticosteroid injections for lateral epicondylitis; a systematic review. Pain. 2002;96:23-40
11. Smidt N, van der Windt DA, Assendelft WJ, Deville' WL, Korthals-deBos IB, Bouter LM. Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: a randomised controlled trial. Lancet. 2002;359:657-662
12. Kleinman M, Gross AE. Achilles tendon rupture following steroid injection: report of three cases. J Bone Joint Surg Am 1983;65:1345'7.
13. Rees JD, Maffulli N, Cook J. Management of tendinopathy. Am J Sports Med. 2009;37(9):1855-1867
14. Ohberg L, Lorentzon R, Alfredson H. Eccentric training in patients with chronic Achilles tendinosis: normalised tendon structure and decreased thickness at follow up.. Br J Sports Med. 2004 Feb;38(1):8-11
15. Hall MP, Band PA, Meislin RJ, Jazrawi LM, Cardone DA. Platelet-rich plasma: current concepts and application in sports medicine. J Am Acad Orthop Surg. 2009 Oct;17(10):602-608.
16. Peerbooms JC, Sluimer J, Bruijn DJ, Gosens T. Positive Effect of an Autologous Platelet Concentrate in Lateral Epicondylitis in a Double-Blind Randomized Controlled Trial: Platelet-Rich Plasma vs Corticosteroid Injection With a 1-year Follow up. AM J Sports Med. Feb 2010, 38:255-62.
17. Mehta S, Watson JT. Platelet-rich concentrate: basic science and clinical applications. J Orthop Trauma. 2008;22(6):432-438.
18. Alsousou J, Thompson M, Hulley P, Noble A, Willet K. The biology of platelet-rich plasma and its application in trauma and orthopaedic surgery: a review of the literature. J Bone Joint Surg Br. 2009;91(8):987-996.
19. Foster, TE, Puskas, BL, Mandelbaum, BR, Gerhardt MB, Rodeo SA. Platelet-Rich Plasma: From Basic Science to Clinical Applications. AM J Sports Med. Nov 2009, 37:2259-72.
20. De Mos M, van der Windt AE, Jahr H, van Schie HTM, Weinans H, Verhaar JAN, van Osch GJVM. Can Platelet Rich Plasma Enhance Tendon Repair? A Cell Culture Study. AM J Sports Med. June 2008. 36:1171-8.
21. Mishra A, Woodall J Jr, Vieira A. Treatment of tendon and muscle using platelet-rich plasma. Clin Sports Med. 2009 Jan;28(1):113-25.
22. Molloy T, Wang Y, Murrell G. The roles of growth factors in tendon and ligament healing. Sports Med. 2003;33:381â394.
23. Virchenko O, Aspenberg P. How can one platelet injection after tendon injury lead to a stronger tendon after 4 weeks? Interplay between early regeneration and mechanical stimulation. Acta Orthop. 2006;77(5):806-812.
24. Kajikawa Y, Morihara T, Sakamoto H, et al. Platelet-rich plasma enhances the initial mobilization of circulation-derived cells for tend-n healing. J Cell Physiol. 2008;215(3):837-845.
25. de Vos RJ, van Veldhoven PL, Moen MH, Weir A, Tol JL, Maffulli N. Autologous growth factor injections in chronic tendinopathy: a systematic review. Br Med Bull. 2010.
26. Bielecki TM, Gazdzik TS, Arendt J, et al. Antibacterial effect of autologous platelet gel enriched with growth factors and other active substances: an in vitro study. J Bone Joint Surg Br 2007;89(3):417-420.
27. Coleman BD, Khan KM, Maffulli N, Cook JL, Wark JD. Studies of surgical outcome after patellar tendinopathy: clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J Med Sci Sports. 2000 Feb;10(1):2-11.
28. Struijs PA, Kerkhoffs GM, Assendelft WJ, Van Dijk CN. Conservative treatment of lateral epicondylitis: brace versus physical therapy or a combination of both. A randomized clinical trial. Am J Sports Med. 2004;32:462-469.
29. de Vos RJ, Weir A, van Schie HTM, et al. Platelet-Rich Plasma Injection for Chronic Achilles Tendinopathy: A Randomized Controlled Trial. JAMA. 2010;303(2):144-149
30. Sampson S, Gerhardt M, Mandelbaum B. Platelet rich plasma injection grafts for musculoskeletal injuries: a review. Curr Rev Musculoskelet Med. 2008 Dec;1(3-4):165-74.
31. Martinez-Gonzalez JM, Cano-Sanchez J, Gonzalo-Lafuente JC, Campo-Trapero J, Esparza-Gomez G, Seoane J. Do ambulatory-use Platelet-Rich Plasma (PRP) concentrates present risks? Med Oral. 2002 Nov-Dec;7(5):375-90.
32. McShane, JM, Nazarian, LN, Harwood, MI. Sonographically guided percutaneous needle tenotomy for treatment of common extensor tendinosis in the elbow. J Ultrasound Med. 2006; 25:1281.
33. McShane JM, Shah VN, Nazarian LN. Sonographically guided percutaneous needle tenotomy for treatment of common extensor tendinosis in the elbow: is a corticosteroid necessary? J Ultrasound Med. 2008 Aug;27(8):1137-44.
34. Housner JA, Jacobson JA, Misko R. Sonographically guided percutaneous needle tenotomy for the treatment of chronic tendinosis. J Ultrasound Med. 2009 Sep;28(9):1187-92.
35. Mautner K, Malanga G, Colberg R. Optimizing Outcomes with Platelet Rich Plasma Injections for Recalcitrant Tendinopathy: A Review. Pain Manage. (2011) 1(6), 523â532.
Return To The Case Studies List.



























{kind=link}
{kind=link}