Working Diagnosis:
Complete isolated avulsion of adductor longus at the origin.
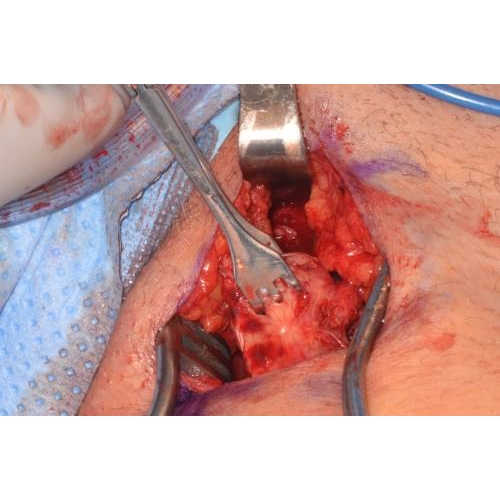
Treatment:
Surgical repair performed using non-absorbable suture anchors to restore normal anatomy. Case Photo #2 Case Photo #3
Outcome:
Successful surgical repair by orthopedics. The post-operative course was complicated by self-resolved incisional hematoma.
He was non-weight bearing on crutches for 4 weeks post-operatively and then transitioned to weight bearing as tolerated with addition of gentle adductor stretching.
Adductor strengthening exercises were added to regimen after 6 weeks and light jogging after 8 weeks. Following 12 weeks of rehabilitation he had full resolution of pain, return of full adductor strength, and was cleared for unrestricted activity.
Author's Comments:
Isolated adductor longus ruptures are an extremely rare injury with few reported cases in the literature. Of the available cases the majority occur at the musculotendinous junction, although some occur distally or as avulsions at the origin. These injuries have been observed in sports that involve kicking or sprinting with rapid changes of direction (ie. soccer, football). The proposed mechanism of injury is a non-contact injury resulting from wide hip abduction with extension and internal rotation causing a strong eccentric contraction of adductors.
Clinically, adductor longus rupture presents with acute groin pain accompanied by a popping sensation and rapid development of edema and ecchymosis in the inner thigh. Physical exam demonstrates adductor weakness with painful passive abduction and resisted adduction. Palpation at the site of adductor longus origin may reveal a tender mass or defect. Diagnosis can be made by ultrasound or MRI.
Due to the rarity of injury there is no established best treatment. Both surgical and non-surgical management have resulted in successful return to play at professional levels of competition. Surgical repair to restore normal anatomy appears to result in full return of objective muscle strength. One case series of NFL players managed non-surgically demonstrated a quicker return to play (6 weeks vs 12 weeks). However,
other studies have shown permanent decrease in adductor muscle strength of unknown functional significance. EMG studies to analyze muscle group contributions during specific activities found that adductor longus primarily provides hip stabilization rather than generating power during sprinting or cutting motions. This may suggest that full anatomical reapproximation of adductor longus may not be vital for even high-level athletic performance.
The majority of reported cases in the literature have been successfully managed surgically with full return to previous activity level, however, more data is required to determine best treatment guidelines. In this case a thorough discussion of the available evidence was conducted with the patient by both Sports Medicine and Orthopedic Surgery providers ultimately resulting in the decision for surgical repair.
Editor's Comments:
While complete adductor longus rupture is rare, it can be readily diagnosed in the setting of a consistent mechanism of injury with a thorough physical exam and appropriate imaging. Good long-term outcomes and return to play are possible with either surgical or non-surgical options, but there are no validated guidelines as little published research exists regarding the ideal treatment recommendations. Complete avulsions have typically been managed surgically with successful return to activity. However, a BMJ report concluded that, "given the overall evidence of conservative management of adductor tears and possible complications associated with surgery... acute adductor tears in the majority should be treated conservatively". Ultimately, the decision should be made on a case-by-case basis between the athlete and sports medicine/orthopedic providers, especially among high level athletes. Developing chronic groin pain with functional limitation is possible if not appropriately treated. Previous groin injury is a risk factor for future groin injury with inadequate rehabilitation the likely underlying factor. An active training exercise protocol for patients with longstanding adductor-related groin pain seems best.
References:
Rizio L, Salvo JP, Schurhoff MR. Adductor longus rupture in professional football players: acute repair with suture anchors. A report of two cases. American Journal of Sports Medicine. 2004;32(1):243-245.
Schlegel TF, Bushnell BD, Godfrey J. Success of nonoperative management of adductor longus tendon ruptures in National Football League athletes. American Journal of Sports Medicine. 2009;37(7):1394-1399.
Quah C, Cottam A, Hutchinson J. Surgical management of a completely avulsed adductor longus muscle in a professional equestrian rider. Case Reports in Orthopedics. 2014.
Thorborg K, Petersen J, Nielsen MB. Clinical recovery of two hip adductor longus ruptures: a case-report of a soccer player. BMC Research Notes;2013(6):205.
Akermark C, Johansson C. Tenotomy of the adductor longus tendon in the treatment of chronic groin pain in athletes. American Journal of Sports Medicine. 1992(20):640-643.
Mann RA, Moran GT, Dougherty SE. Comparative electromyography of the lower extremity in jogging, running and sprinting. American Journal of Sports Medicine. 1986;14(6):501-510.
Neptune RR, Wright IA, Van den Bogert AJ. Muscle coordination and function during cutting movements. Medicine & Science in Sports & Exercise. 1999;31 (2);294-302.
Dimitrakopoulou A, Schilder E. Acute avulsion of the fibrocartilage origin of the adductor longus in professional soccer players: A report of two cases. Clin J Sport Med. 2008;18:167-169.
Lohrer H, Nauck T. Proximal adductor longus tendon tear in high level athletes: a report of three cases. Sportverletz Sportschaden. 2007;21(4):190-194.
Banks DBA, MacLennan I, Banks AJ. Adductor longus ruptures in elite sportsmen-pitfalls of surgical repair: a report of two cases. BMJ Case Rep. 2013.
Arnason A, Sigurdsson SB, Gudmundsson A, Holme I, Engebretsen L, Bahr R. Risk factors for injuries in football. Am J Sports Med. 2004;34:5S-16S.
Hagglund M, Walden M, Ekstrand J. Lower reinjury rate with a coach-controlled rehabilitation program in amateur male soccer - a randomized controlled trial. Am J Sports Med. 2007;35:1433-1442.
Holmich P, Uhrskou P, Ulnits L, Kanstrup IL, Nielsen MB, Bjerg AM, Krogsgaard K. Effectiveness of active physical training as treatment for long-standing adductor-related groin pain in athletes: randomised trial. Lancet. 1999;353:439-443.
Return To The Case Studies List.


























{kind=link}
{kind=link}